




Chronic rhinosinusitis (CRS) is a chronic sinus disease that affects between 5% and 12% of the general population.1–3 Despite substantially impacting the patient’s quality of life, it often remains underdiagnosed and undertreated.1
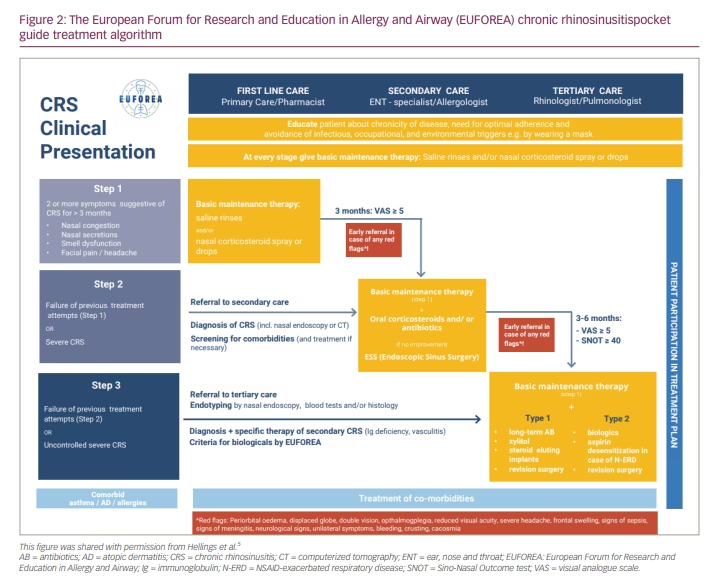
The European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) recently published a CRS pocket guide providing a simplified clinical care pathway for diagnosing and managing CRS (Figure 1).4 The pocket guide features a new, easy-to-use treatment algorithm and diagnostic checklist encouraging cross-speciality care and patient education. It aims to provide healthcare professionals and patients with streamlined practical guidance and improved knowledge of CRS (Figure 2).5
In this expert interview, Prof. Peter Hellings discusses the need for succinct and easy-to-use guidelines in CRS, how implementing the pocket guide will affect clinical outcomes, and the importance of disseminating the guide amongst all stakeholders, including pulmonologists, allergologists, immunologists and patients.
Q. Why does chronic rhinosinusitis often remain underdiagnosed and undertreated?
CRS is often considered a trivial disease with a self-limiting nature, meaning that patients with CRS tend to heal by themselves within a couple of days or weeks, as with the common cold. However, this is not the case. If patients continue to show symptoms beyond 12 weeks, such as nasal obstruction, smell loss, headache, facial pain, or nose and throat secretions, they must be properly diagnosed. However, a primary care physician cannot always be offered a proper diagnosis because they might not be able to perform a nasal endoscopy. A nasal endoscopy needs to be conducted by an ear, nose, and throat (ENT) surgeon or doctor, who can evaluate not only the nasal but also the sinus cavities. In patients with CRS, a nasal endoscopy may reveal signs of on-going sinus disease, such as swelling, polyps and pus. Delays in diagnosis occur because CRS is considered a non-life threatening, trivial disease and also because most primary care physicians cannot perform a nasal endoscopy. Another reason for the delay could be that patients tend to underestimate the severity and burden of their disease. We believe that it is important for patients to receive a timely and proper diagnosis to allow them to access the best possible therapeutic strategy, such as lifestyle measures, local treatments and nasal douching. Lifestyle measures and simple solutions can be implemented to prevent the disease from becoming severe or chronic and irreversible.
Q. What guidelines currently exist for chronic rhinosinusitis, and what are their limitations in terms of barriers to diagnosis and treatment?
Several national and international guidelines are available; however, the problem with several of these guidelines is that they do not always reflect the daily reality of the physicians treating the disease. Furthermore, many of them are very lengthy; for example, the the 2020 European Position Paper on Rhinosinusitis (EPOS2020) guidelines take up more than 400 A4 pages.3 Therefore, it can be difficult for primary care physicians to understand the guidelines in detail, to find the position of every single patient within the treatment algorithm and to determine the best next step for an individual patient. There are a multitude of guidelines, and a simplified uniform guideline is needed. Thus, EUFOREA joined forces with different organizations and bodies to create a novel, simplified guideline. We developed this EUFOREA pocket guide for CRS, which includes a novel treatment algorithm and guideline.4 This treatment algorithm is simple and comprehensive and also reflects the reality of every patient consulting an ENT physician, primary care physician or tertiary care specialist on the treatment options for CRS. We recommend simple options as first-line care and more systemic treatments, as well as sinus surgery, as second-line care. In patients whose CRS remain severe and uncontrolled, we may recommend oral steroids or biologics, or we might consider revision sinus surgery.
Q. Please could you give us a brief overview of the chronic rhinosinusitis pocket guide and its aims?
The EUFOREA CRS pocket guide not only focuses on pharmacotherapy but also stresses the importance of educating patients about lifestyle and hygiene measures that could positively impact their disease and the organs of the sinuses.4 We recommend that patients avoid irritants and occupational triggers that play a role in the chronicity and severity of CRS. Furthermore, the EUFOREA treatment algorithm explains that the physician and the patient should work together to design the best possible therapeutic plan. Often, patients will already have tried more than one local or systemic treatment option for CRS. Therefore, it is important that the patient gets an insight into the different options and decides on the next step of care together with a physician. For example, when a patient with CRS has had sinus surgery, which is often unsuccessful in one out of two patients, we need to decide what the next step would be in the case that symptoms persist or that symptoms come back after 1, 3 or 5 years. At that moment, we need to educate the patient about the indication of biologics, which are new treatment options that are very beneficial for patients with CRS and nasal polyps, and about revision sinus surgery, which could also be beneficial but is not always successful and has a major risk of severe complications. We need to discuss the benefits and drawbacks of different therapeutic approaches with the patient to give them a better understanding of the treatment options, the expectations of each treatment option, and what could be the best next step for them. Importantly, this EUFOREA pocket guide also focuses on the comorbidities of CRS; indeed, we know that if you only focus your treatment plan on CRS, you may neglect comorbidities such as asthma and respiratory allergies. These comorbidities need to be properly treated to achieve the best possible outcome for CRS. Lastly, it is important that we understand and recognize aspirin intolerance in patients with CRS because a failure to do so might lead to suboptimal treatment and rapid recurrence of CRS after sinus surgery. All of these key facts, recommendations and considerations are included in this pocket guide, which is available on the EUFOREA website.4
Q. Please could you describe the diagnostic checklist and chronic rhinosinusitis algorithm?
Patients suffering from headaches, nasal obstruction, smell loss, facial pain and secretions might have CRS. Therefore, it is important to consider a diagnosis of CRS in patients who present with two or more of these symptoms. Whenever CRS is susptected, a physician might start empiric treatment with nasal douching and/or nasal corticosteroids and evaluate the effect of the treatment for 6–8 weeks. Depending on the level of disease control, we might continue the treatment, and some patients may need to be referred to an ENT specialist. If symptoms do not respond well to treatment after 6–8 weeks, we would recommend referring to an ENT specialist for a nasal endoscopy. Then, depending on the diagnosis and the patient’s history, the ENT specialist can fine tune and adapt the treatment according to the needs of the patient. However, it is important to take the holistic approach of signed entities and make sure to not neglect to consider why CRS might occur. Some patients may be affected by an immune disorder; in these cases, we need to check the immune status of the patient. In other patients, we may need to evaluate the dental status to make sure there is no odontogenic origin of CRS. We may need to screen patients for allergies and other comorbidities, such as asthma, or for orbital issues and other problems. In the EUFOREA pocket guide, we explain that it is important to consider why some patients with CRS may need to be seen by an ophthalmologist, a pulmonologist, an allergologist or an immunologist.4 It is vital to consider the full spectrum of comorbidities in patients with CRS to achieve the best possible outcome.
Q. How will implementing the chronic rhinosinusitis pocket guide affect clinical outcomes?
So far, there have been no studies investigating the contribution of the EUFOREA pocket guide to the field of CRS. However, in other domains, the availability of guidelines, especially simplified guidelines, has been shown to speed up diagnosis and also help patients to access the right care earlier in the disease process than without guidelines. A survey in the UK has shown that timely treatment might prevent patients with CRS from developing asthma, demonstrating that timely treatment holds preventive potential.6 A European survey conducted by EUFOREA found that the majority of patients with CRS wait for an average of 3–5 years to see an ENT specialist for a nasal endoscopy.7 It is humbling and unfortunate that the majority of patients experience such a delay in receiving proper diagnosis and treatment, as timely treatment is needed for them to have a normal quality of life. We should not underestimate the burden of CRS; a study has shown that the quality of life of patients with severe uncontrolled CRS suffers to the same extent as that of patients with conditions such as severe rheumatoid arthritis and type 2 diabetes.8 Notably, the majority of patients with CRS also have smell loss; moreover, when you lose your sense of smell, you often also lose some of your capacity to taste. We should not neglect the fact that patients with severe CRS often lose two out of five of their senses. At EUFOREA, we have a patient advisory board where many of the patients express how it feels to live with severe CRS and how it feels to live without a sense of smell or taste. It is very emotional to hear the testimonials of patients. They describe the impairment to their quality of life as living their life in black and white rather than a colourful, bright life full of good-tasting foods and pleasant smells, such as the smell of their children or relatives. I think this is part of the quality of life that, unfortunately, most patients with CRS miss out on.
Q. To whom will the EUFOREA chronic rhinosinusitis pocket guide be available?
We believe that we have a unique guideline that can be understood by primary care physicians, ENT specialists, pulmonologists, allergologists and even paediatricians. It is vital that all stakeholders in the field of CRS can observe and evaluate the recommended treatment options. At this moment, the EUFOREA team is focusing on the dissemination of the pocket guide and the pocket guide is being translated into several European and other languages, which is great. We currently have the Spanish and Catalan versions, and versions in other languages will soon become available. We also plan to create a plain language version of the pocket guide so that patients with CRS can have access to information about treatment options and be empowered. This is crucial, because we need plain language information and plain language educational material to help patients understand the treatment options, what they should consider and what they should discuss with their physician to make sure they get access to the best possible care.



