




Paediatric sleep-disordered breathing
Sleep-disordered breathing (SDB) is defined as the disruption of normal respiration and ventilation while asleep.1 SDB encompasses multiple sleep disturbances, ranging from mild snoring to obstructive sleep apnoea (OSA).1,2 OSA is characterized by episodic partial or complete obstruction of the upper airway, with associated desaturations, awakenings or arousals from sleep.3 Common symptoms include snoring, nocturnal gasping, witnessed apnoeas and daytime somnolence.4,5 OSA affects 1–4% of children worldwide, with incidence increasing over time.6–8 When untreated, paediatric OSA is known to negatively affect outcomes and quality of life.9 OSA has been linked with neurocognitive and behavioural disturbances in paediatric patients, including learning difficulties, attention disorders, poor school performance, hyperactivity, aggression, moodiness and antisocial behaviours.10–14 Paediatric OSA may also be associated with cardiovascular disease and hypertension.1,8,15–17
Evaluation and diagnosis of paediatric obstructive sleep apnoea
The gold standard for the diagnosis of OSA in children is in-laboratory overnight polysomnography (PSG).3 However, current research efforts are in place to determine the efficacy of less invasive, more readily accessible diagnostic methods in the paediatric population.2,18 The American Academy of Sleep Medicine defines paediatric obstructive apnoea events as a reduction in peak airflow by ≥90% of pre-event baseline with an associated respiratory effort.19 A hypopnoea event is defined as a decrease in the peak signal by ≥30% from baseline nasal pressure for at least two breaths in association with either a ≥3% oxygen desaturation or an arousal.19 OSA is diagnosed using the apnoea–hypopnoea index (AHI), which is the average number of apnoeas and hypopnoeas per hour of sleep.19 The most commonly accepted definition of OSA severity is mild OSA corresponds to an AHI ≥1 and <5, moderate with an AHI of 5–10 and severe with an AHI of ≥10.3,8,20
Pathophysiology
Lymphoid tissue in Waldeyer’s ring serves as part of the immune system, positioned in the oropharynx and nasopharynx to initiate immune responses towards antigens entering the body.20,21 This tissue is most active between 3 and 10 years of age, leading to an associated peak in size during this period with subsequent age-related involution.20,22 To date, there have been no studies demonstrating a significant impact on immune function after the removal of the adenoids and/or tonsils to manage SDB.23
Certain populations are at a higher risk of developing OSA than others. In the USA, upwards of 60% of children with obesity have comorbid OSA.24,25 The aetiology of this relationship is likely multifactorial, but the co-occurrence of obesity and adenotonsillar hypertrophy may have a cumulative effect on narrowing the oropharyngeal airway.26,27 Other risk factors for paediatric OSA include craniofacial anomalies and neuromuscular disorders.8,28,29
Trisomy 21: An at-risk population
A well-studied, unique population with high rates of OSA is patients with Down syndrome (DS).30 Overall, 55–80% of children with DS have OSA.31,32 Hill et al. found that 14% of children with DS had moderate-to-severe OSA and 59% had mild-to-moderate OSA.33 Some characteristic features of DS, such as obesity, baseline hypotonia and altered craniofacial anatomy, including midface hypoplasia and macroglossia, place them at a higher risk of the disease.33,34 OSA may be associated with severe ramifications in this population. Breslin et al. identified an association between OSA, reduced cognition and lower verbal intelligence quotient in a paediatric DS cohort.35 Due to the high incidence of OSA in these patients, the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) recommends screening all children with DS for OSA by overnight PSG before 4 years of age.20 Unfortunately, patients with DS are more likely to have disease persistence after initial therapy with adenotonsillectomy (AT).36–38 Reasons for this are discussed later in this article.
Treatments
Adenotonsillectomy
In children, the most common cause of OSA oropharyngeal obstruction is adenotonsillar hypertrophy.1,20 The AAO-HNS guidelines support surgical management via AT as the first-line treatment for appropriate children with OSA diagnosed using PSG.20 AT is also indicated for children who demonstrate signs of obstructive SDB with adenotonsillar hypertrophy and clinical signs of comorbid conditions, such as growth retardation, enuresis and school/behavioural issues, which may improve after surgery.20
Surgical removal of the adenoids and palatine tonsils often results in significant improvements in respiratory parameters, including the AHI, obstructive apnoea and hypopnoea indices and minimum oxygen saturation.39 Success rates of AT approaches 80% in certain populations.40–42 AT has also been associated with improvements in behaviours, such as aggression, attention and hyperactivity, and in the quality of life.9,43
While highly efficacious in developmentally typical children, AT has lower efficacy in children with DS.36 The literature suggests that 30–50% of children with DS have persistent OSA after AT.44 In addition, these children suffer higher complication rates post-operatively. Cottrell et al. demonstrated that 78/251 (31.5%) of children suffered a post-operative complication needing medical attention, most commonly respiratory issues (53.8%), poor oral intake (37.2%) and bleeding (17.9%).45 These findings were echoed by Goldstein et al.46 In this setting, additional or alternate therapies may be considered.
Continuous positive airway pressure
Continuous positive airway pressure (CPAP) is the mainstay of treatment for adult patients with OSA and is an option for children who are not appropriate surgical candidates for AT.47 It can also be considered in children with persistent OSA after AT.47,48 CPAP is delivered nasally or oronasally via a mask and stabilizes the upper airway by providing positive pressure that exceeds the pressure of the collapsing intraluminal oropharyngeal space.49 Studies have highlighted the benefits of positive airway pressure (PAP) therapy in managing SDB.50,51 However, adherence to PAP is a barrier to its efficacy in both adult and paediatric populations, leading to persistent, untreated disease.52,53 PAP adherence is not as well defined in children as in adults.54 However, the most common definition of PAP adherence utilized for children is the adult definition: use of PAP ≥4 hours per night for 70% of nights during 30 consecutive days.55
Weiss et al. found that less than half of the children with OSA were using CPAP for >4 hours a night.56 Children with caregiver support show improved compliance, and the medical team’s engagement via family-based education programmes on CPAP improves adherence.54,57 Additionally, it has been found that younger children (primary school age versus middle/high school age), those with higher baseline AHI and those with neurocognitive disorders better tolerate PAP.58
Notably, non-invasive ventilation, including PAP, is an option for children with DS who have persistent OSA after AT or who are not candidates for surgical management.48,59 However, PAP is less effective in children with DS than in developmentally typical children.60 Despite improved adherence to PAP, children with DS have poorer clinical outcomes compared with non-DS counterparts, namely persistent AHI elevations and mask leaks.60,61 Therefore, it is important to continue re-evaluating these children to ensure appropriate treatment responses. If the result is unsatisfactory, other treatments may be required.
Non-positive airway pressure upper airway approaches in obstructive sleep apnoea
There are additional non-surgical and surgical options for the management of persistent OSA. Non-surgical approaches work to expand the oropharyngeal airway to reduce obstruction. Common options include rapid maxillary expansion and oral appliances providing maxillary advancement.62–65 Although individual studies have shown promise, the data are lacking to definitively comment on these options in children.66 Surgical alternatives also aim to increase the size of the oropharyngeal airway. These include oromaxillofacial procedures, namely maxillomandibular advancements and mandibular distraction osteogenesis, or neurosurgical procedures, such as fronto-facial monobloc advancement.63,67–69 Tongue base reduction and lingual tonsillectomy can be considered in cases with obstruction at these sites.70,71 Expansion sphincter pharyngoplasty is another procedure aimed at improving oropharyngeal obstruction in children with persistent OSA.72,73
The only cure for persistent OSA is a tracheostomy, typically performed by otolaryngology or paediatric surgery physicians.48,74 Discussion on which of these treatments are most appropriate requires a multidisciplinary sleep medicine team and shared decision-making between the team and the caregivers.63 Further details about these treatments are outside the scope of this article. A list of the mentioned options and their efficacy can be found in Table 1.40–42,44,48,54,67–69,71,72,74–79
Table 1: Comparison of paediatric hypoglossal nerve stimulation with other obstructive sleep apnoea treatment modalities40–42,44,48,54,67–69,71,72,74–79
|
Procedure/device |
Success rate |
|
Paediatric HGNS |
At least 50% reduction in AHI in paediatric patients75 |
|
AT |
|
|
Continuous positive airway pressure |
|
|
Oral appliances |
May have efficacy; data are lacking in children77,78 |
|
Maxillomandibular advancement |
*Surgical success rate: 85.5%; surgical cure rate: 38.5%67 |
|
Mandibular distraction osteogenesis |
|
|
Tongue base reduction |
48.5% reduction in AHI71 |
|
Lingual tonsillectomy |
AHI <1, success rate 17%; AHI <5, success rate 51%79 |
|
Expansion sphincter pharyngoplasty |
Cure rates: AHI <1, 64%, AHI <2, 72% and AHI <5, 60%72 |
|
Tracheostomy |
Considered curative48,74 |
*Data are derived from adult populations.
AHI = apnoea–hypopnoea index; AT = adenotonsillectomy; DS = Down syndrome; HGNS = hypoglossal nerve stimulation; OSA = obstructive sleep apnoea.
Hypoglossal nerve stimulation
The upper airway consists of 23 pairs of muscles that are state-dependent, exhibiting reduced activity upon sleep onset.80–82 Of these, the genioglossus is readily accessible, and its role in OSA has, thus, been extensively studied.83 The genioglossus is an extrinsic muscle of the tongue, originating from the superior mental spine and inserting at the tip and dorsum of the tongue and into the body of the hyoid bone.84 It is innervated by cranial nerve 12 and supplied by the lingual arteries. Importantly, the genioglossus works to maintain airway patency by stabilizing the upper respiratory tract.85,86
Efforts to increase the upper airway muscular output, such as myofunctional therapy and playing woodwind instruments, for the treatment of OSA have been attempted.87,88 These therapies target the oral cavity and oropharyngeal structures to strengthen dilator muscles of the upper airway, which relax during sleep and thus result in soft tissue collapse in the throat. Patency of the pharyngeal airway, which lacks intrinsic support, may be improved with oropharyngeal exercise.88,89
Proof of concept
Despite varying therapeutic success rates of oropharyngeal exercises on OSA resolution, they provided the rationale for the hypoglossal nerve stimulation (HGNS) device. Studies in both animal models and humans were performed to test this idea.
Animal models served as a proof of concept for hypoglossal stimulation for the treatment of OSA.90,91 Stimulation of the hypoglossal nerve decreased upper airway collapsibility via contraction of musculature, leading to improved patency and dilation. Schwartz et al. found that stimulation of the proximal trunk of the hypoglossal nerve, which primarily innervates the genioglossus, reduced pharyngeal collapsibility.91 Stimulation of the hypoglossal nerve, via activation of the genioglossus muscle, was more effective than stimulation of the strap muscles and other lingual muscles.92 Later, it was determined that action by both tongue protrudor muscles (genioglossus) and retractors (styloglossus and hyoglossus) occurs when respiratory drive increases, supporting co-stimulation of both muscle groups to stabilize the airway during sleep.93,94
Simultaneously, various forms of stimulation were attempted in humans. Miki et al. placed percutaneous electrodes into the genioglossus muscle in six patients during overnight PSG.95 The authors noted that the stimulation of this muscle significantly decreased the incidence of apnoea episodes, promoted deeper sleep and did not have any serious side effects.95 Schwartz et al. used transoral intramuscular electrodes to stimulate the hyoglossus, styloglossus and genioglossus muscles, noting the different effects on airway patency by each muscle group.96 Some authors similarly used fine-wire electrodes directly into the genioglossus, while others developed methods for stimulating the nerve directly.97,98 This allowed for the activation of both the protrudor and retractor muscles for best outcomes. As data accumulated, both in animal and in human studies, there was strong evidence for direct HGNS in support of airway adequacy during sleep.99
Implantation trials
Prior to its approval by theUS Food and Drug Administration (FDA), several studies were conducted to evaluate the feasibility and efficacy of fully implanted HGNS devices. The initial studies were performed in adults. In 2001, Schwartz et al. implanted a tripolar cuff electrode for HGNS.100 The device was placed in eight adults, confirming the feasibility of the procedure and therapeutic benefits in OSA via stimulation of the entire distal nerve.100 The authors noted reduced AHI and oxyhaemoglobin desaturations after intervention with unilateral hypoglossal activation.100 Subsequently, a similar study was performed with more patients, finding comparable results lasting for at least 1 year.101
With the knowledge that branches of the hypoglossal nerve could be directly isolated and stimulated to move the genioglossus and improve airway obstruction, technology and techniques advanced to place the cuff electrode more distally, thereby targeting the protrudor muscles.97,102 This adjustment was supported in multiple studies, demonstrating similar efficacy.103–106
Several issues with these devices were appreciated. Eastwood et al. noted that 71% of participants experienced one or more adverse events from the implantation surgery, including numbness, pain or skin irritation at the incision site.104 In addition, 67% of participants experienced therapy-related complications, including abrasions on the tongue surface and tongue muscle fatigue.104 However, these events were of short duration and resolved in all cases.104 Most studies cite low rates of similar complications.99 Overall, the pilot studies suggested that implantation was well tolerated with therapeutic efficacy for the management of OSA. Therefore, definitive trials were warranted.
Clinical trials
The Stimulation Therapy for Apnea Reduction Trial (STAR; ClinicalTrials.gov identifier: NCT01161420) was pivotal in assessing the outcomes of unilateral HGNS in adult patients with OSA.107 This was a multicentre, prospective, single-group cohort study of patients with OSA intolerant to CPAP. The primary outcome measures were AHI and oxygen desaturation index (ODI) changes with implantation. Secondary outcomes included quality-of-life assessments as well as percentage of sleep time with oxygen saturation <90%. Inclusion criteria were patients 22 years or older who were intolerant to CPAP with a body mass index (BMI) of 32 kg/m2 or less and AHI between 20 and 50 events per hour. Exclusion criteria were tonsillar hypertrophy and collapse of palatal tissues on pre-operative drug-induced sleep endoscopy (DISE). The study included 126 patients, 66% of whom saw a reduction of at least 50% in baseline AHI at 1 year. The authors noted that at the 12-month follow-up, repeat PSG revealed a median AHI reduction of 68% and an ODI reduction of 70% from baseline. In addition, 23 patients were selected for randomized therapy withdrawal, thereby serving as their own controls. These patients had return of their OSA despite a reduction in AHI the week prior, during the use of the device, further confirming its efficacy. Patients also reported improvement in secondary outcomes, namely quality of life, snoring and daytime sleepiness.107 Treatment responses were sustained at 3 and 5 years after implantation with minimal risk.102,108 A subsequent meta-analysis found that all available devices performed similarly, indicating equivalent treatment success as well as potential generalizability of the aforementioned results.109
Three medical device companies have conducted human trials with hypoglossal nerve stimulators. The Inspire® Upper Airway Stimulation system (P130008/S039; Inspire Medical Systems, Inc., Maple Grove, MN, USA) received FDA approval in 2014, with post-market trials using the device.110,111 The long-term safety of the Genio® system (Nyxoah SA, Mont-Saint-Guibert, Belgium) in adult patients with OSA will soon be assessed in a clinical trial (A prospective, open-label, multicentric extension study to assess the long-term safety of the Genio® system in study subjects who have been implanted with the Genio® implantable stimulator [IS] for the treatment of OSA in adult patients; ClinicalTrials.gov identifier: NCT05939141).112
Procedure
By maintaining a stiffened tongue and tongue protrusion, the HGNS device opens the airway and reduces airway collapse during sleep.113 The Inspire® Upper Airway Stimulation system is composed of a respiratory sensing lead, impulse generator (IPG) and stimulation lead. The device is controlled by an external remote control. The respiratory-sensing lead detects the respiratory cycle phase and activates the impulse generator upon inspiration; the impulse generator then sends an electrical impulse to the stimulation lead on the hypoglossal nerve, causing tongue protrusion.83 107,114 Figure 1 provides a flow diagram of this process.114
Figure 1: Flow diagram of the mechanism of action of the hypoglossal nerve stimulation114
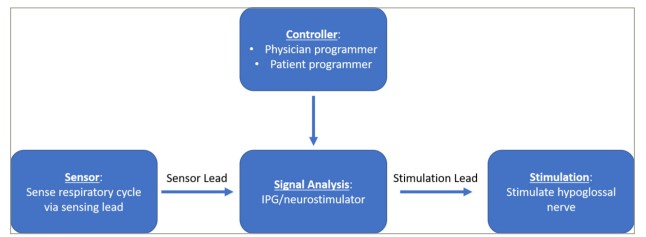
IPG = implantable pulse generator.
Reproduced with permission from Vanderveken et al.114 (http://creativecommons.org/licenses/by-nc/4.0).
The HGNS device was originally introduced as a right-sided, three-incision approach to limit noise from the cardiovascular system and accommodate existing cardiac implantation devices.115–117 This strategy involved one incision for the stimulator lead midway in the right submandibular region, a second incision for the IPG at the right anterior chest wall and a third incision for the respiratory-sensing lead along the fifth or sixth intercostal space at the lateral chest.115 Kent et al. eliminated the need for the third incision site by placing the respiratory sensory electrode behind the IPG.118 Due to the reduced intraoperative time and post-operative pain, the FDA approved the two-incision, right-sided implantation in March 2021.116,119 The two-incision technique has also been successfully conducted in left-sided implantation and should be considered if right-sided implantation is contraindicated.120
Devices are typically activated 1 month following placement. Patients are required to repeat a PSG to optimize the voltage settings for upper airway patency throughout sleep several months after surgery, with additional routine follow-up to ensure treatment success.110
Hypoglossal nerve stimulation in children
As mentioned previously, patients with DS are uniquely at risk for OSA, and disease persistence, after initial treatment. A majority (55–80%) of children with DS have OSA.31,32 In this population, the pathophysiology is multifactorial and related to several anatomic features, including generalized hypotonia, macroglossia, midface hypoplasia, small tracheal calibre and lingual tonsil hypertrophy.121 It is estimated that only 16–33% of children with DS and OSA have resolution of their OSA after AT.121,122 Oftentimes, the site of residual obstruction is at the base of the tongue or may be due to pharyngeal collapse and oropharyngeal crowding associated with concomitant obesity and/or lingual tonsillar hypertrophy.121 It has also been shown that 63% of patients with DS and persistent OSA have obstruction from glossoptosis, a feature that can be improved with HGNS. Therefore, this technology was applied specifically to children with DS in the setting of CPAP intolerance.36
Several case reports have shown the success of HGNS in adults with DS, suggesting expanded indications for the device. Van de Perck et al. reported a case of an adult patient with DS, severe OSA and CPAP intolerance who underwent HGNS.123 They were found to have a 63% decrease in AHI and a 77% decrease in ODI 6 months after HGNS device implantation, with an average device usage of 9.4 hours per night.123 A case series of three adults with DS and OSA showed strong adherence to the use of HGNS at an average of 57.3 hours per week and overall reductions in the titrated AHI.124
With these studies in mind, implantation was then attempted in children with DS. Diercks et al. implanted the first six paediatric HGNS devices in 2018.125 Participants (aged 12–18 years) had DS and severe OSA (AHI >10 events/hour) despite prior AT.125 In all patients, the implant was well tolerated and effective in significantly improving their OSA.125 At 1-year follow-up, patients showed an 85% reduction in AHI, with four children having an AHI <5 events/hour and two children with AHI <10 events/hour.125 The authors also reported a significant improvement in quality of life with the use of the HGNS device in these patients, as measured by the OSA-18 questionnaire.125 Caloway et al. evaluated the safety and efficacy of HGNS in 20 nonobese children and adolescents (aged 10–21 years) with DS and severe OSA.126 These patients had prior intolerance to CPAP after previous AT.126 The authors found that HGNS therapy was both safe and effective, with a median percentage reduction in titration AHI of 85% and a change in OSA-18 scores by 1.15 points, indicating a moderate clinical change in the quality of life.126 A systematic review and meta-analysis of efficacy and adverse effects of HGNS in adolescents with OSA and DS identified nine studies, with a total of 106 patients.127 This study found that HGNS significantly reduces the AHI as well as improves the quality of life in patients undergoing the procedure.127 At this time, there is an ongoing clinical trial (Effects of hypoglossal nerve stimulation on cognition and language in Down syndrome and obstructive sleep apnea; ClinicalTrials.gov identifier: NCT04801771) involving 57 adolescents and young adults (aged 10–21 years) with DS and moderate-to-severe sleep apnoea post-AT for 12 months after HGNS device implantation.128 The study will evaluate changes in cognition and language after therapy with the HGNS device.
Clinical indications
FDA approval for the Inspire® Upper Airway Stimulation system (P130008/S039) was originally granted in May 2014.111,129 In 2023, FDA approval expanded and now includes (1) people with moderate-to-severe OSA (15 ≤ AHI ≤ 100) aged 22 years and older who cannot tolerate PAP or bi-level PAP and who do not have complete blockage of the soft palate; (2) people aged 18–21 years with moderate-to-severe OSA (15 ≤ AHI ≤ 100) and (3) people aged 13–18 years with DS and severe OSA (10 ≤ AHI ≤ 50) who are not AT candidates and have been considered for all alternative treatments.111,129 Table 2 provides the complete FDA inclusion criteria for HGNS.129–131 To date, there are limited studies in children as the device was only recently approved.129–131 It is expected that there will be a growing body of literature on children, which likely will result in further expansions for the indications and patient eligibility.
Table 2: US Food and Drug Administration inclusion criteria for hypoglossal nerve stimulation129–131
|
|
2014130,131 |
2023129 |
||
|
Parameter |
|
|
||
|
Age |
>18 years |
22+ years |
18–21 years |
13–18 years with DS |
|
AHI |
15 ≤ AHI ≤ 65 events/hour |
15 ≤ AHI ≤ 100 events/hour |
10 ≤ AHI ≤ 50 events/hour |
|
|
BMI |
<32 kg/m2 |
<40 kg/m2 |
||
|
Central/mixed apnoeas |
<25% of total events |
<25% of total events |
||
|
DISE findings |
No complete concentric collapse at the palate |
No complete concentric collapse at the palate |
||
|
Failed PAP |
Yes |
Yes |
Yes |
|
|
Other |
|
|
|
|
Central or mixed apnoeas must comprise <25% of the total AHI score.
AHI = apnoea–hypopnoea index; AT = adenotonsillectomy; BMI = body mass index; DISE = drug-induced sleep endoscopy; DS = Down syndrome; PAP = positive airway pressure.
Complications
Overall, HGNS therapy is well tolerated. The STAR trial reported no serious complications, rehospitalizations or infections from the procedure.107 Two participants required repositioning of the neurostimulator due to discomfort. Less serious adverse events related to tongue discomfort resolved with continued use of the HGNS device.107 No long-term complications were reported in a cohort of 600 patients followed for 1 year after implantation.132 It should be noted that patients with HGNS undergoing external electrical cardioversion should be counselled on potential device malfunction.133 Additionally, patients with chronic lower respiratory diseases may be at an increased risk of intraoperative pneumothorax and pleural effusion and must be counselled accordingly.134
Paediatric trials parallel adult trials in their low complication rates. Diercks et al. reported that two patients experienced perioperative adverse events, including irritation of the chest incision and poor pain control, which were addressed with antibiotics and improved pain regimens.75,125 Jayawardena et al. indicated no major complications among 23 patients implanted with the HGNS device.135 Other cited complications include tongue or oral pain/discomfort, oral ulcers, surgical-site rash/cellulitis and cheek swelling.127
Some unique paediatric considerations include the potential for device displacement during puberty, the need for battery replacement every 10 years and the potential benefit of adjustments in surgical technique.75,135 Further research is needed to fully evaluate these possibilities.
Hypoglossal nerve stimulation outcomes
To date, the success rate for HGNS is best established in adults, with a quoted rate of 66%.107 Factors contributing to surgical success are being further elucidated. Ong et al. found that patients with complete anterior–posterior or lateral soft palate and/or epiglottic collapse are at risk of HGNS failure.136 Complete concentric collapse at the velum is a known contraindication for implantation, and in this study, patients with this pattern were excluded from implantation.129,136 Chao et al. noted lateral oropharyngeal collapse and significantly elevated preoperative AHI (49.4 ± 19.6 versus 36.9 ± 18.8, p=0.05) as risk factors for poor surgical success.137 Xiao et al., interestingly, did not find any association between DISE patterns of collapse, but instead noted Mallampati III/IV and Friedman Tongue Position IV as factors that led to mildly decreased response.138 Lee et al. noted that patients with lower pre-operative PAP requirements (<8 cm H2O) had a greater response rate to HGNS.139 Seay et al. similarly found that lower PAPs during a DISE were associated with HGNS responders when compared with non-responders.140
Researchers and surgeons are expanding the use of HGNS outside of the FDA approval criteria (Table 2). Sarber et al. reported the implantation in such patients with a success rate of 67%, which is similar to the 1-year STAR trial results at 66%.141 The need to better characterize appropriate patients for this procedure, with additional data points outside of the FDA approval, is currently being investigated.130
Summary
OSA is common in the paediatric population, with higher rates in at-risk groups. AT is the first-line treatment for the majority of children, and management of persistent OSA after AT is nuanced. HGNS has recently expanded therapeutic options for patients with refractory OSA, including children and adolescents with DS. To date, this procedure has proven effective and well tolerated across multiple clinical trials. Continued studies will likely expand eligible paediatric, and adult, candidates for HGNS.


