




Sarcoidosis is a chronic systemic disease of unknown origin that is characterized by the formation of noncaseating granulomas in various organs, predominantly in the lungs. Granulomas are the pathologic hallmark of the disease and usually occur in the bronchial submucosa allowing bronchoscopic diagnosis by the use of a variety of diagnostic modalities to assess the airway in sarcoidosis.1,2 The bronchial mucosa in sarcoidosis may appear normal, inflammation with miliary or large nodules containing noncaseating granulomas may be present, and, less commonly, yellowish nodules with a cobblestone appearance may be observed.2,3 Occasionally, endobronchial granulomas form a mass-like lesion that can obstruct the bronchial lumen.4
Endobronchial involvement is common and granulomas are found anywhere in the respiratory tract with positive endobronchial biopsy findings in up to 40 to 70 % of patients.3–7 Bronchial biopsy may identify granulomas in approximately a third of cases with a normal mucosa because the granulomas are usually located in the airways. In the presence of mucosal lesions, diagnostic yield of bronchoscopic biopsies may be as high as 75 %.3–6
Although endobronchial disease is frequent in sarcoidosis, data concerning the clinical characteristics and prognosis of such patients is missing. The clinical features and prognosis of endobronchial disease have not been reported in the literature. Data relevant to patients with endobronchial sarcoidosis are limited with proximal bronchial involvement leading to bronchial stenosis or narrowing. The prognostic implications of endobronchial disease have only been assessed as a determinant of a factor causing stenosis.5,7
In this review, the main aim is to discuss the clinical features of endobronchial disease in regard to prognosis and extrapulmonary organ involvement in sarcoidosis.
Endobronchial Involvement in Sarcoidosis
Endobronchial involvement is not an uncommon sequela of sarcoidosis. Bronchoscopy can provide valuable information regarding the type, extent, and location of endobronchial disease for visible lesions and thereby allows histopathologic confirmation. Even when the airway mucosa appears normal, the diagnostic yield of bronchial biopsy may reach to 30 %.
Sarcoidosis confined to the airway may present with cough, wheeze, and dyspnea out of proportion to the parenchymal radiologic changes.8 Bronchial stenosis or narrowing are more frequently detected later in the course of the disease, mainly affecting the proximal parts of the
segmental or lobar bronchi. However, superficial endobronchial lesions of sarcoidosis may not lead to significant symptoms. Although the superficial granulomas remain clinically silent, they may lead to notable changes in the laboratory findings. The prognosis and extrapulmonary organ involvement in these patients are also significantly different from those without histopathologically evident endobronchial sarcoidosis.9
The classic anatomic distribution of sarcoidosis is along the bronchovascular bundles and lymphatics.10 Therefore, the bronchial mucosa is often involved in sarcoidosis, 40 % of patients with stage I and approximately 70 % of patients with stage II and III have noncaseating granulomas in bronchial biopsy specimens.2,10,11 Due to the airway centered granulomas, even with a normal appearing mucosa, sarcoid granulomas are identified by bronchial biopsy in approximately a third of cases, while diagnostic yield rises to 75 % in the presence of mucosal abnormalities.3–7 Shorr and colleagues have shown that 71 % of sarcoidosis patients had bronchial abnormalities and even in patients with normal appearing airways, granulomas can be identified in 30 % of cases.3 Patients with endobronchial disease may show significant clinical differences from those without airway involvement. The laboratory findings including serum angiotensin-converting enzyme (ACE), calcium and 24-hour urinary calcium are significantly different. Extrapulmonary organ involvement and the disease prognosis are also more severe in patients with endobronchial disease exhibiting distinctive and contrasting features. The most frequent bronchoscopic finding of endobronchial disease was miliary infiltration (38 %) followed by nodular (26 %) and erythematous (18 %) lesions while 16 patients (16.3 %) had mixed type of lesions.9
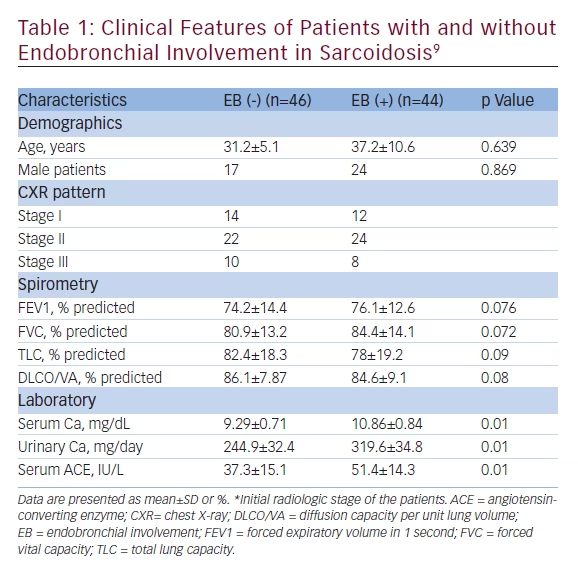
Previous studies have primarily investigated the clinical implications and treatment of bronchial stenosis due to endobronchial granulomas. Few studies have emphasized the functional and bronchoscopic features of endobronchial sarcoidosis but they have not reported the clinical and prognostic consequences of superficial mucosal involvement.3,5,7,12 They included a small number of patients with stenotic bronchial lesions. The authors have provided a broad description, evaluation and treatment options for bronchial stenosis or narrowing due to sarcoidosis. Chambellon et al. have also emphasized the need for early treatment, since a delay in treatment beyond 6 months did not lead to improvement in the lesion.7 Yanardag et al. have defined the clinical features of endobronchial involvement and its correlation with prognosis.9 In these patients, extrapulmonary organ involvement was more frequent compared with patients without endobronchial disease. Pulmonary function tests and diffusion capacity per unit lung volume (DLCO/VA) were not significantly different between the two groups. ACE, serum, and urinary calcium levels were higher than subjects without endobronchial lesions (see Table 1).
Endobronchial sarcoidosis appears to be a significant factor for progressive and advanced disease. These patients had approximately four times a worse prognosis than patients without endobronchial involvement. The severe prognosis is probably associated with the high granuloma burden caused by endobronchial lesions. This finding is also supported by the raised levels of serum ACE, serum, and urinary calcium reflecting the high granuloma burden.9 In the Yanardag study, endobronchial lesions did not lead to stenosis or narrowing and were superficial or had a normal mucosal appearance.9 Presence of endobronchial involvement may implicate a severe and a progressive disease. These findings emphasize the significance of bronchoscopic biopsies in regard to prognosis and thereby a progressive disease. The above result is unique because previous studies have reported that only proximal stenotic bronchial lesions would be an indicator of serious disease.3–6,13,14 Endobronchial disease carries a potential risk for progressive disease in sarcoidosis patients in regard to a worse prognosis and a more frequent extrapulmonary organ involvement. Advanced pulmonary sarcoidosis develops in 5–6 % of all patients and radiologically evident pulmonary fibrosis develops in approximately 10 %.15,16 No study has comprehensively surveyed all potential risk factors for persistent sarcoidosis. While no specific risk factors for advanced pulmonary disease have been identified, numerous factors like old age, lupus pernio, splenomegaly, or multiple organ involvement have been defined for progressive and/or advanced disease.17–21 The Yanardag study is exclusive for demonstrating that endobronchial involvement is a significant risk factor for progressive and advanced disease.9 Treatment of sarcoidosis is based on the premise that suppression of granuloma formation results in preservation of organ function and minimization of advanced disease or long-term fibrosis,12,21–23 which may be considered as the supporting evidence for these findings. The prognostic differences between patients may be due to the variable kinetics of granuloma formation in each individual.
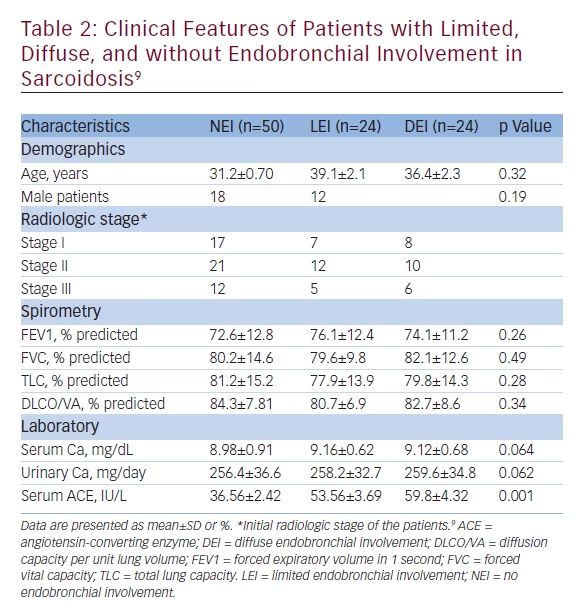
Tetikkurt et al. have reported that patients with no endobronchial involvement (NEI), limited endobronchial involvement (LEI), and diffuse endobronchial involvement (DEI) have shown significant differences in regard to clinical features (see Table 2), extrapulmonary organ involvement, and prognosis. Pulmonary function tests, DLCO/VA, serum and urinary calcium levels were not significantly different between the three groups in this study while ACE was significantly higher in the LEI and DEI groups than the NEI group. This finding implicates a higher granuloma burden in the LEI and DEI patients. The prognosis was approximately seven times worse in the DEI group while it was four times worse in the LEI group than the NEI group. Extrapulmonary organ involvement was more frequent and severe in the LEI and DEI group compared with the NEI patients contributing to the worse prognosis. The higher the granuloma burden, caused by diffuse endobronchial disease, in a patient the worse the prognosis is and the extrapulmonary organ involvement is more severe. This is supported by the fact that patients with DEI showed the most unfavorable clinical implications compared with the LEI and NEI groups.9 Extrapulmonary organ involvement may also depend upon the burden of noncaseating granulomas in sarcoidosis.
Although sarcoidosis that is progressive or chronic does not always eventuate in fibrotic disease, presence of endobronchial involvement whether limited or diffuse, identified by bronchoscopy, may be a significant marker for severe prognosis. Apart from the diagnosis, fiber optic bronchoscopy should be performed in every sarcoidosis patient for the identification of severe prognosis with multiple biopsies taken from different sites even if the bronchial mucosa appears normal. The effect of limited or diffuse endobronchial sarcoidosis leading to more severe extrapulmonary organ involvement and more progressive disease is supported by the fact that current treatment options are targeted at suppression of granulomas.9,12,23
Endobronchial involvement, either limited or diffuse, appears to be a potential risk factor for advanced disease in sarcoidosis. On the other hand, endobronchial disease may also lead to severe organ involvement in sarcoidosis. As bronchoscopic diagnosis of endobronchial lesions is an easy procedure, pulmonologists should routinely use bronchoscopy and obtain multiple mucosal biopsies for the diagnosis of endobronchial sarcoidosis for identifying patients under a potential risk for a worse prognosis. Bronchoscopy will thereby be useful for the diagnosis of endobronchial involvement necessitating a close follow-up for the early identification of progressive disease in such patients without any delay in treatment. In conclusion, endobronchial disease identified by bronchoscopy is a significant determinant of a worse prognosis and severe extrapulmonary organ involvement in sarcoidosis.


