




Chronic rhinosinusitis (CRS) is a heterogeneous inflammatory disease of the nose and paranasal sinuses that is prevalent worldwide, affecting 10–12% of adults.1,2 It is phenotypically classified by the presence or absence of nasal polyps. Chronic rhinosinusitis with nasal polyposis (CRSwNP) is estimated to affect up to 4% of the population, and consists of multiple endotypes that are defined by the multiple and often overlapping mechanistic pathways leading to mucosal inflammation.3–5
The estimated annual cost of managing CRS in the United States is $22 billion.6 First-line management for CRSwNP relies on medical therapy with saline irrigations and intranasal corticosteroids. Short courses of oral steroids can be used as adjuncts. Surgical intervention is usually considered in cases that are refractory to medical management. However, recurrent disease following surgery remains a risk: 7–15% of patients who have undergone an initial operation require additional surgery.7,8 Despite medical and surgical management, many patients experience persistent or recurrent symptoms as assessed by tools such as the Sino-Nasal Outcome Test-22 (SNOT-22),9 and evidenced by sinonasal disease on nasal endoscopy and/or computed tomography (CT).
Recently, immunotherapeutics have become an option for add-on treatment of refractory CRSwNP, targeting the type 2 inflammatory biomarkers that are characteristic of CRSwNP pathophysiology. The type 2 inflammatory pathway upregulates the production of cytokines interleukin (IL)-4, IL-5 and IL-13, which subsequently promote the activation of eosinophils, basophils and mast cells.10 This response is also used by the immune system against helminthic infections, but can also drive other non-infectious inflammatory processes, such as asthma, atopic dermatitis and CRSwNP.11 Based on their ability to target various components of the type 2 inflammatory pathway, biologic agents have improved clinical outcomes for patients with these inflammatory conditions. Current biologic therapies approved for use in CRSwNP include dupilumab, a monoclonal antibody against the α subunit of the IL-4 receptor that is critical for the downstream signalling and effects of IL-4 and IL-13, and omalizumab, a monoclonal antibody that targets free immunoglobulin (Ig)E.12–16
As a hallmark cytokine of type 2 inflammation and highly prevalent in nasal polyp tissue, IL-5 has become another treatment target for CRSwNP.17–19 Patients with CRS and comorbid allergic rhinitis and/or bronchial asthma are more likely to have elevated tissue eosinophils than controls or patients without these comorbid conditions.20 Though primarily produced by activated T-helper cells, IL-5 is also produced by mast cells, eosinophils and natural killer cells. Binding of IL-5 to its receptor on eosinophils promotes their activation, differentiation, survival and degranulation. The critical role that IL-5 plays in type 2 inflammation has already resulted in the development of anti-IL-5 biologic therapies for the lower airway, which have shown clinical benefit in patients with severe eosinophilic asthma.21–23 Mepolizumab, for example, is a monoclonal antibody designed to bind to free circulating IL-5. Given the similar inflammatory pathways that can been seen in asthma and CRSwNP, anti-IL-5 therapies have also been closely studied for clinical efficacy and safety in CRSwNP.10,24
Mepolizumab has been the subject of recently completed phase II and III clinical trials for CRSwNP treatment, and in July 2021, received approval from the US Food and Drug Administration (FDA) for use in patients with CRSwNP.25 This review aims to summarize the efficacy and safety of mepolizumab for CRSwNP refractory to medical and surgical management, as reported in the landmark clinical trials.
Pharmacology of mepolizumab
Mepolizumab is a fully humanized monoclonal IgG1κ antibody that binds to free circulating IL-5, preventing it from interacting with its receptor. Subcutaneously administered, mepolizumab has 64–75% bioavailability, and when intramuscularly administered has 81% bioavailability. The volume of distribution is approximately 49–93 mL/kg body weight. It is metabolized widely in the body by proteolytic enzymes and excreted non-renally. The elimination half-life is around 20 days.26–28 In previous studies of mepolizumab in asthma, a change in route of administration from intravenous to subcutaneous was approved for add-on maintenance therapy.22 Thus, a change in dosing from 750 mg intravenously every 4 weeks to 100 mg subcutaneously every 4 weeks is also observed across the studies included in this review.
Clinical efficacy in eosinophilic diseases
Mepolizumab is approved for use in severe eosinophilic asthma, hypereosinophilic syndrome (HES) and eosinophilic granulomatosis with polyangiitis (EGPA). In severe eosinophilic asthma, the DREAM (NCT01000506) and MENSA (NCT01691521) trials showed that add-on maintenance therapy with either intravenous or subcutaneous mepolizumab was well tolerated and efficacious in reducing the risk of asthma exacerbation.21,23 In a secondary analysis of the data from both trials, this efficacy was found most clinically significant in patients with a baseline blood eosinophil count of ≥150 cells/μL.23 Mepolizumab also improved quality-of-life measures in the MUSCA (NCT02281318) trial.29 Furthermore, mepolizumab was well tolerated in long-term use up to 4.5 years in patients with severe eosinophilic asthma in the COLUMBA (NCT01691859) and COSMEX (NCT02135692) trials.30,31
A post hoc analysis of the MUSCA and MENSA (NCT01691521) trials for severe eosinophilic asthma evaluated the presence of comorbid nasal polyposis on physical examination and chart review, and the potential use of mepolizumab for CRSwNP was analysed through the change in sinonasal symptom-related quality of life during the study durations.32 This effect on CRSwNP-related symptoms was assessed by SNOT-22. In the two trials analysed, nasal polyposis was present at baseline in 19% of patients. The mean SNOT-22 score for patients with nasal polyposis was reduced by 13.7 points from baseline after 24 weeks of mepolizumab add-on therapy, compared with a decrease of 1.9 points with placebo. Furthermore, while mepolizumab significantly decreased the rate of asthma exacerbation overall, the effect was more pronounced in patients with comorbid nasal polyposis than those without comorbid nasal polyposis. Additionally, the improvement in quality of life related to upper and lower airway symptoms with mepolizumab was greater in patients with nasal polyposis than those without nasal polyposis.32
Mepolizumab has also proven safety and efficacy in HES and EGPA. For example, mepolizumab was associated with a steroid-sparing effect and reduction in disease flares in two clinical trials for patients with HES.33,34 These findings were sustained with long-term use up to 6 years.35 In a case series of patients with HES treated with mepolizumab, one patient with comorbid asthma and CRSwNP also reported improved nasal congestion and had improved polyposis on examination.36 Finally, mepolizumab improved rates of remission in patients with EGPA in a single clinical trial and post hoc analysis.37,38
Clinical efficacy in chronic rhinosinusitis with nasal polyposis
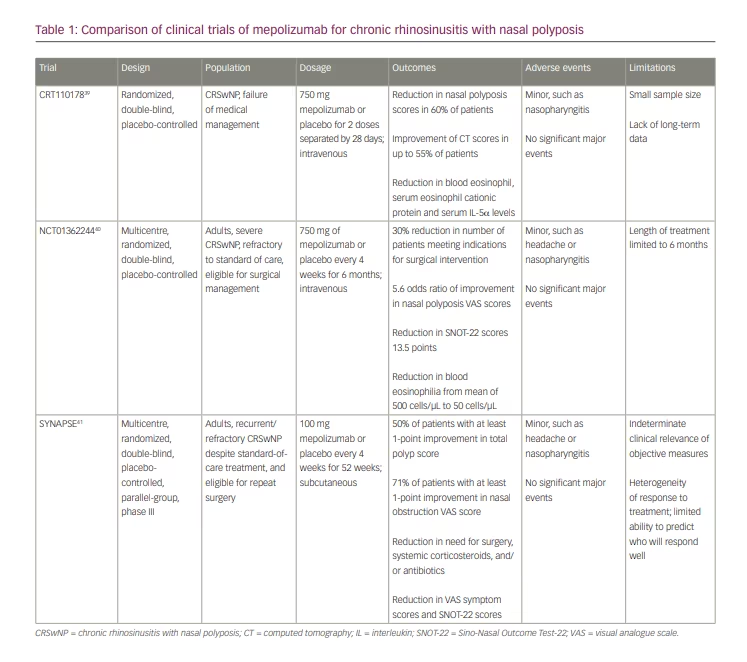
The clinical efficacy of mepolizumab in CRSwNP has been evaluated in published phase II and III trials. Most recently, a phase III trial (SYNAPSE; NCT03085797) assessed the efficacy and safety of mepolizumab in CRSwNP treatment, after which mepolizumab gained FDA approval. These clinical studies are summarized below as well as in Table 1.39–41
CRT110178
Design
Study CRT110178 (Mepolizumab, a humanized anti-IL-5 mAb, as a treatment option for severe nasal polyposis) was a randomized, double-blind, placebo-controlled, phase II trial in 30 patients with either primary nasal polyposis (grade 3 or 4) or recurrent nasal polyposis after surgery.39 Patients were included if they had failed the standard of care for CRSwNP, which was defined according to the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS).3 Using a visual analogue scale (VAS) of 0–10, patients rated the severity of sinonasal symptoms that included nasal blockage, discharge, facial pain/pressure, reduced sense of smell and sleep disturbance. Nasal endoscopy findings and use of rescue medications were also analysed. Patients were randomly assigned to receive either two doses of 750 mg of intravenous mepolizumab or placebo. The doses were given 28 days apart, and the patients were followed for 48 weeks. The primary endpoint was the change in total nasal polyp score after 8 weeks of treatment, which was measured as the sum of right and left nasal passage scores on nasal endoscopy. Secondary endpoints were changes in CT scores, nasal peak inspiratory flow, symptom scores, blood eosinophils and cytokine levels. Safety was assessed by adverse events, vital signs, symptom checks, physical examination and blood analysis.
Results
Almost half of the 30 patients included had atopic disease, and 43% of them had asthma. For the primary endpoint, total polyp score at 8 weeks was significantly reduced in 60% of patients treated with mepolizumab compared with 10% of those receiving placebo. There were no particular patient factors identified between patients who responded to treatment, including baseline total polyp scores and IL-5 levels. CT scores were improved in 55% of the mepolizumab-treated patients versus <20% of placebo-treated patients, with good agreement between the three CT investigators. A high dropout rate was noted in this study; however, it is noteworthy that the time to dropout was significantly longer in patients treated with mepolizumab than with placebo. Laboratory measures, such as blood eosinophil, serum eosinophil cationic protein and serum IL-5α levels were significantly reduced in the mepolizumab-treated group. A trend towards improvement in CT scores, symptom scores and nasal peak inspiratory flow was also detected in the mepolizumab-treated group, though it did not reach statistical significance. Markers in nasal secretions were also not significantly different between the two groups. In total, 53% of patients experienced adverse events during the 48-week study period, none of which was noted to be significantly associated with treatment, and the most frequent were the common cold.
Limitations of this study include a small sample size and lack of long-term data. In summary, 55–60% of patients treated with mepolizumab had improved objective measures of CRSwNP.
NCT01362244
Design
NCT01362244 (Reduced need for surgery in severe nasal polyposis with mepolizumab: Randomized trial) was a randomized, double-blind, placebo-controlled multicentre, phase II study of 105 adult patients with severe bilateral nasal polyposis who were eligible for surgery.40 Patients were treated with either 750 mg of mepolizumab or placebo intravenously every 4 weeks for 6 doses. Patients were required to have received intranasal corticosteroids for 3 months prior to the first dose of mepolizumab, and intranasal steroids were continued during the study. The primary endpoint was the number of patients no longer requiring sinus surgery at week 25 based on nasal polyp score and nasal polyposis severity. Secondary endpoints included need for surgery at each time point, change in nasal polyposis severity score, change in endoscopic nasal polyp score, individual symptom VAS scores, peak nasal inspiratory flow and olfaction, as assessed by the Sniffin’ Sticks Screening-12 test. Safety was assessed by adverse events, vital signs, electrocardiograms and clinical laboratory testing.
Outcomes
Approximately 78% of patients enrolled in the study had comorbid asthma. At the end of the study period of 25 weeks, 30% of patients treated with mepolizumab no longer met indications for surgery, a statistically significant reduction compared with the 10% of patients receiving placebo who no longer required surgery. This reduction was first seen at week 9 and was sustained through 25 weeks.
There was also a statistically significant improvement in nasal polyposis severity VAS scores compared with placebo, with an odds ratio of 5.6 in patients treated with mepolizumab. Mean individual VAS scores were also significantly improved in the mepolizumab group compared with the placebo group at week 25. Of note, the specific symptoms of rhinorrhoea and nasal obstruction were decreased beginning at week 5, and mucus and loss of smell were significantly decreased at week 9. The reduction in these symptoms was sustained throughout the trial period. Furthermore, mean SNOT-22 scores were improved by 13.5 points at week 25 compared with placebo, indicating that there were both statistically and clinically significant effects.
A post hoc analysis revealed no association between baseline eosinophil counts and achieving at least a 1-point reduction in endoscopic nasal polyp scores at week 25. In terms of mean peak nasal inspiratory flow, a mean increase of 26.7% flow was noted in patients treated with mepolizumab versus placebo. These results were statistically significant. There was a trend, though not statistically significant, for reduced olfaction scores in those treated with mepolizumab versus placebo. In terms of laboratory results, a post hoc analysis showed blood eosinophil counts decreased from a mean of 500 cells/μL to 50 cells/μL at week 25. Such a reduction was not detected in the placebo group.
Adverse events leading to discontinuation were similar between the mepolizumab and placebo groups. The most common adverse events were headache and nasopharyngitis. Vitals and laboratory evaluations were also similar between the two groups. There was a decrease in mean leukocyte counts in the mepolizumab group, which was sustained throughout the course of treatment; however, it did not appear to be clinically significant.
Limitations of this study include lack of long-term data and use of intravenous therapy.
SYNAPSE
Design
SYNAPSE (Mepolizumab for chronic rhinosinusitis with nasal polyps (SYNAPSE): a randomised, double-blind, placebo-controlled, phase 3 trial) was a multinational, parallel-group trial performed across 93 institutions from May 2017 to December 2018.41 The patient population included 407 adults with recurrent, refractory bilateral nasal polyposis deemed to have failed both medical and surgical management. The patients were randomized to receive either 100 mg mepolizumab subcutaneously or placebo every 4 weeks for a total of 52 weeks. They also continued standard-of-care treatment and had to have at least 8 weeks of intranasal corticosteroid sprays prior to screening. Coprimary endpoints were change from baseline in endoscopic nasal polyp score and mean nasal obstruction VAS score from week 49 to week 52. Secondary endpoints included time to first nasal surgery during the study period, systemic corticosteroid requirement, antibiotic requirement, changes in SNOT-22 scores, number of patients no longer requiring surgery, changes in University of Pennsylvania Smell Identification Test scores and changes in blood eosinophil counts. Safety was assessed by number of serious adverse events, local injection site reactions, systemic reactions, changes in haematological and metabolic laboratory values, 12-lead electrocardiogram and immunogenicity.
Outcomes
In this study, approximately 71% of patients had asthma. Both coprimary endpoints were met, as 50% of patients receiving mepolizumab had at least a 1-point improvement in total polyp score, and 71% of patients had an improvement of at least 1 point in the nasal obstruction VAS score. Treatment with mepolizumab appears to be of clinical benefit, as there was a statistically significant reduction in the number of patients requiring nasal surgery, in addition to reduced numbers of required systemic corticosteroids and antibiotics. Importantly, from the patients’ perspective, there was a significant improvement in symptoms overall, as there was a statistically significant reduction in symptom VAS scores, including composite and loss of smell, and SNOT-22 scores.
Adverse events were similar between groups. The most commonly reported minor adverse events included nasopharyngitis, headache, epistaxis and sinusitis. There were no treatment-related major adverse events noted.
An important limitation that applies to this study, NCT01362244 and CRT110178 is the inability to determine a clinically relevant reduction in nasal polyp size. There is currently a void in the literature concerning the minimum change in polyp size – even when standardized by VAS or when reviewers are blinded to all other clinical aspects – that correlates with a meaningful clinical improvement. A second limitation of the SYNAPSE study was that there was limited ability to determine which patient clinical characteristics would predict a favourable or lack of response to treatment with mepolizumab. The only exception was patients with blood eosinophilia; however, more research is required to determine which clinical factors, if any, can assist in predicting which patients will respond favourably to mepolizumab.
Regulatory affairs in use of mepolizumab for nasal polyposis
Mepolizumab was previously approved for severe eosinophilic asthma, HES and EGPA. In July 2021, it received approval for use in CRSwNP.25 However, its cost should be considered, as patients with CRSwNP already have substantial annual costs, particularly when compared with patients with CRS without nasal polyposis. For instance, average annual cost of prescriptions for patients with CRSwNP was estimated to be $3,169 for oral corticosteroids, $3,085 for macrolide antibiotics, and the average cost of endoscopic sinus surgery was $13,532.8,42 A recent cost analysis comparing dupilumab with endoscopic sinus surgery found surgery to be more cost effective.43 According to the Institute for Clinical and Economic Review, the annual cost of mepolizumab for patients with asthma is approximately $32,500 per year prior to any discounts.44 As data regarding the use of mepolizumab in CRSwNP continue to accumulate, it will be vital to assess both the clinical efficacy and cost effectiveness of oral steroids, antibiotics, surgery and biologic therapy. Since its FDA approval, mepolizumab has the potential to be covered by insurance companies, like other biologic therapeutics already approved for CRSwNP. Cost of management is a significant component of shared decision-making, especially when considering disease severity, risks and benefits associated with various medical and surgical therapies, prior therapeutics and patient preference.
Conclusion
Mepolizumab is a biologic agent that has demonstrated efficacy in various inflammatory diseases, including asthma, HES and EGPA, and, most recently, CRSwNP. It has now gained FDA approval for treating patients with CRSwNP. Mepolizumab reduces nasal polyp disease burden from both subjective and objective standpoints. Furthermore, CRSwNP treatment with mepolizumab reduces the number of prescriptions for systemic corticosteroids and antibiotics, which have well-known adverse effects. The adverse events related to mepolizumab are relatively mild.39–41 Future trials will need to explore the efficacy of mepolizumab with the other FDA approved biologics for CRSwNP. At the time of this writing, there is a trial comparing dupilumab and omalizumab.45 Future research is also needed to define the role of biologics in the overall treatment strategy for CRSwNP.


